What is PKD?
Polycystic Kidney Disease (PKD) is a genetic disease that causes the kidneys to grow multiple cysts. As these cysts grow larger, blood flow becomes strained and can lead to tissue damage and scarring. Eventually this can lead to kidney failure. Since PKD affects roughly 1 in every 800 people and accounts for 5-10% of dialysis patients, it is important to understand how the disease may affect you too.
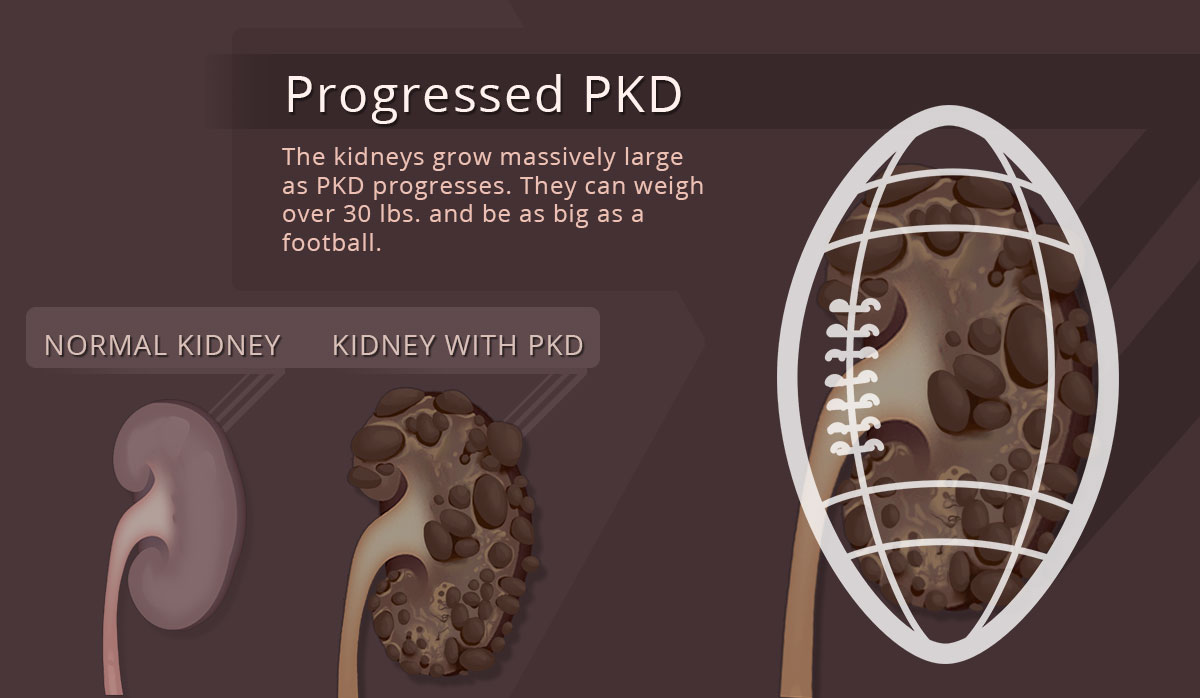
What PKD Looks Like

How do you get PKD?
PKD is usually inherited from one or more of your parents. The cysts form because genes in your DNA have mutated and caused cells to grow/multiply rapidly when they shouldn’t. There are two major forms of PKD—it’s important to understand the difference!
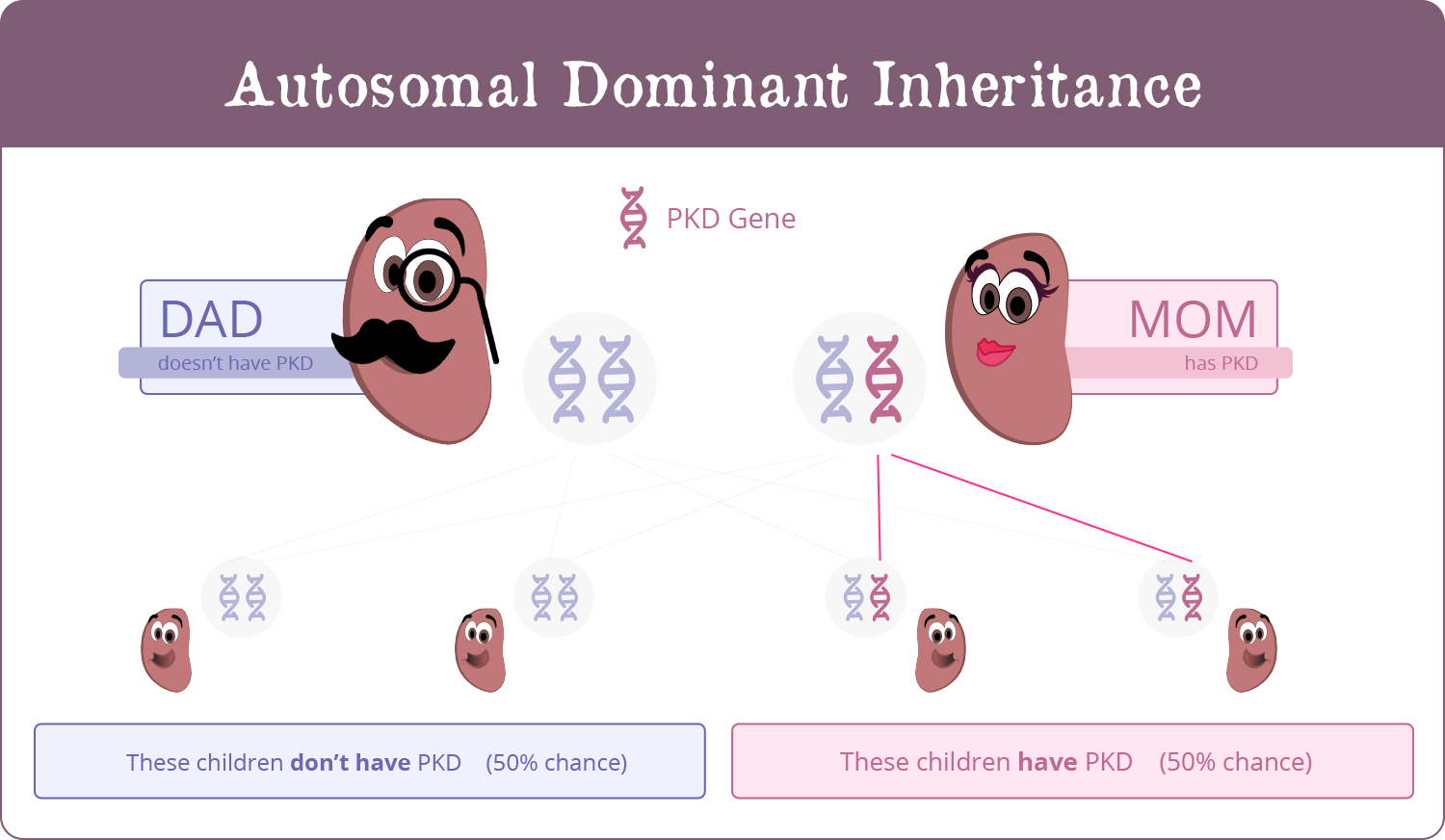
PKD 1: Autosomal Dominant
Most common, usually comes from one parent
Each child of an affected parent has a 50% chance of getting the disease
Does not skip generations: If child of an affected parent doesn’t get it, grandchildren won’t either
PKD 2: Autosomal Recessive
Much less common (1 in 20,000 people)
Mutated gene has to be present in both parents, then child has 25% chance of getting it
Usually diagnosed in infancy, sometimes up to adolescence in mild cases
Okay, so there are different types. Should I care which one I have?
Absolutely! PKD 1 is aggressive and more common (85% of families). The average age for needing dialysis here is 55 years. On the other hand, PKD 2 is milder, often presents later in life and may not be diagnosed at all. The average age for needing dialysis is 69 years.
What’s the average timeline of PKD’s progression?
The disease can only be found through a kidney ultrasound, so you should be tested if you have family history. The disease is 99% specific and “at risk” individuals with PKD usually follow these patterns:
- Up to 30 years old: 2 cysts in each kidney
- Age 30-60: 4 cysts in each kidney
- 60+ years of age: 8 cysts in each kidney
If an “at risk” individual has negative ultrasounds at 20 years and 30 years of age, the likelihood of disease inheritance is below 10% and 5% respectively. There are stricter criteria for those with no family history of PKD.
What should I look out for in case I have PKD?
- High Blood Pressure
- Flank & abdominal pain due to kidney swelling
- Blood in urine (cysts can fill with blood & burst)
- Localized pain from infection (requires antibiotic therapy)
- Kidney stones
Unfortunately, you’ll likely get cysts in many other organs as well, so keep an eye out for the following:
- Liver cysts – Very common! The liver may become enlarged and lead to leg swelling and shortness of breath.
- Intracranial aneurysm (ICA) – translation – ‘a brain aneurysm’
- Pancreatic Cysts
- Aneurysm of the Mitral Heart Valve leading to ‘prolapse’ and ‘regurgitation’ – translation – a ‘leaky valve’
- Diverticuli or ‘outpouchings’ of the colon
- Hernias
An intracranial aneurysm in an aneurysm of one of the tiny blood vessels in the brain is one of the complications of PKD. This is an enlarged and dilated blood vessel of the brain which has a chance of rupturing leading to a brain hemorrhage You must get screened if you have a family member with an aneurysm. The bigger they are, the greater the chance of them rupturing.
Helpful hint: PKD tends to cluster in families.
And screening is very important even if you don't have symptoms
Ultrasound of the kidneys is usually the initial modality used for screening and diagnosis. Ultrasound is usually used for screening because it is safe, effective, and inexpensive. It is less reliable in younger individuals hence genetic diagnosis using DNA analysis and/or other imaging tests can be performed when we need a definitive diagnosis
![]()